
With the warnings this week in Canada and the United States about the risks of dosing errors with vitamin D drops, I thought it was an appropriate time to discuss dose measurement as barrier to science-based care. Dosing errors are the among the most common and most preventable causes of adverse drug events in children. Why children? Drugs for children are often in liquid form for ease of measurement and administration. Typically dosed based on milligrams per kilogram, liquid formulations allow us to (in theory) deliver the exact dose that’s appropriate. But measurement isn’t always easy or intuitive. What’s the best way to measure 2.5mL (half a teaspoon)? How easy is it to confuse teaspoons (5mL) and tablespoons (15mL)? And what instructions should health professionals give parents and caregivers to ensure they can measure and administer a dose accurately? Despite the prevalence of dosing errors, there is little evidence telling us what health professionals, or parents, can do better. Until now.
In a study by Yin et al in Archives of Pediatric and Adolescent Medicine, the authors set out to determine what works, and what doesn’t, when it comes to measuring liquid medications for children. If you’re a parent, you’re probably familiar with measuring out medications. It could be over-the-counter drugs like Tylenol, Motrin and Advil, or prescription products like antibiotics. When measuring a liquid, formulation-specific issues such as viscosity (thickness) and surface tension affect the way a liquid behaves. The delivery instrument of choice should compensate for these factors, so the correct dose is administered. In health care settings, the oral syringe is preferred as many of these factors are minimized. But what about in the hands of consumers?
The Study
The study design was simple but effective. Parents were enrolled from a pediatric clinic. All were instructed to measure 1 teaspoon (5mL) of a medication (acetaminophen – Tylenol) using six different measurement methods (links are sample images):
- A dosing cup with printed markings (capacity 15 mL or one tablespoonful)
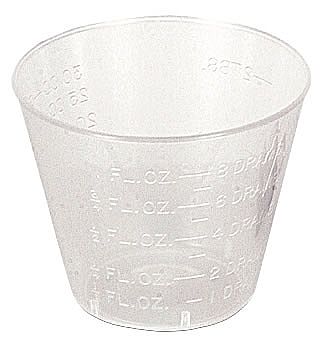
- A dosing cup with etched markings (capacity 30 mL or two tablespoonfuls)
- A dropper (capacity 5 mL)
- A dosing spoon (capacity 10 mL)
- An oral syringe (capacity 5 mL)
- A oral syringe with a bottle adapter (allows the drug to be easily drawn up directly from the bottle) (capacity 5 mL)
Each participant measured using all devices, but they were presented in random order. The measured dose was compared (by weight) with a reference dose drawn up with an oral syringe. Literacy was also assessed using the Newest Vital Sign test, to see what influence that might have on measurement practices. Sociodemographic and child health status information were also collected.
The investigators defined an appropriate dose as one that contained no more that 120% of the expected dose. A small error was 120% to 140%, and a large error was anything more than 140% of the target 1 tsp (5 mL) dose.
The Results
302 subjects were recruited; they were mainly female (95%), Hispanic (80%), and non-US born (76%). About half were high school graduates (51%) and the majority were predicted to have a high likelihood (41%) or possible likelihood (38%) of limited literacy.
Underdoses with all devices were virtually nonexistent. Excess doses, on the other hand, were common. The worst product was the printed dosing cup, where only 30% of parents could measure a dose accurately. The etched dosing cup was a bit better, at 50%. The dropper had the most accurate dosing, with 94% measuring correctly. The syringe was 91%, and the dosing spoon was 86%.
When literacy was examined, it was negatively correlated with dose measurement accuracy. That is, caregivers with lower literacy were more likely to make “large errors” with the different dosing instruments. These errors were far more common with the dosing cups, however.
The Bottom Line
All the science in the world to arrive at an evidence-based, individualized treatment isn’t that useful if parents can’t measure the correct dose. So what does this study tell us? Cups don’t work well, especially among those with more limited literacy. My personal take is that this isn’t just a problem to those with limited literacy. Imagine a sleep-deprived parent trying to measure out a medication in the middle of the night without turning up all the lights – it’s a plausible scenario that could potentially raise the risk of an error. Measurement devices with a volume capacity closest to the correct dose reduce the risk of excessive dosing. Oral syringes are the gold standard for accuracy and when practical, should probably accompany all prescriptions. If cups are used for over-the-counter products like Tylenol, clear indicator lines can improve dose accuracy and minimize the risk of inadvertent overdose.
Reference
![]()
Yin HS, Mendelsohn AL, Wolf MS, Parker RM, Fierman A, van Schaick L, Bazan IS, Kline MD, & Dreyer BP (2010). Parents’ medication administration errors: role of dosing instruments and health literacy. Archives of pediatrics & adolescent medicine, 164 (2), 181-6 PMID: 20124148

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
If cups are used clear indicator lines can improve dose accuracy and minimize the risk of inadvertent overdose.
My dad worked in a pharmacy that had a large customer base of non-English speaking or elderly persons with poor eyesight.
He used to make a mark on the cup or syringe – a big black mark with a permanent marker – at the correct dose. Then he would say, in English or bad Spanish, “Fill it to the line for each dose. Do not use anything else to measure this medicine. Throw the cup/syringe away when the medicine runs out. I will give you a new one with the refill.”
My experience with cups is that sometimes the label is above the line, sometimes below the line, and sometimes the label is next to the line. As a native English speaker with high literacy, cups were difficult. The hollow handle spoons had less variation, although my daughter got one stuck on her finger once requiring a trip to the emergency room when none of my ideas for removing it worked.
It’s not just knowing how to measure a dose — there are also lots of potential errors because parents confuse “mg” with “mL”. I always stress to patients that they must read the product label — so that they know how many “mg” there are per “mL” of product. Then we discuss the appropriate dose (in mg) and the volume of medication required for a dose of this specific product. I always tell patients that there may be several brands of a particular medication, which may contain different concentrations of active ingredient. As well, there are several product lines that use confusingly similar brand names — yet the different products contain a multitude of active ingredients….leading to errors in product selection.
Pingback: Good Idea, Bad Execution: Dosing Errors, A Preventable Harm « Science-Based Pharmacy