
One of the recurrent themes in alternative medicine is the practice of simplifying complex medical conditions, and then offering up equally simple solutions which are positioned as still being within the realm of science. This approach allows the practitioner to ignore all of the complexity and difficulty of practicing real medicine, yet offer nostrums that, on first glance, can sound legitimate. Science-y, even.
I’ve discussed this before in non-science-based approaches to food intolerances, whether it’s using clinically useless IgG blood tests, or declaring the universal dietary enemy to be gluten. David Gorski elaborated on the same theme recently at Science-Based Medicine in the context of cancer treatment, contrasting the simplistic views of alternative medicine purveyors with the facts of cancer research. Cancer is stunningly complex – each of the hundreds of different variants of the disease. I’m always amazed when I speak with oncologists about how treatment regimens have been established. They describe how the results of dozens of clinical trials, led by different trial groups around the world have each contributed to establishing the current “best” regimens for each cancer: the appropriate drugs, doses, intervals and treatment intensities. Good evidence speaks all languages, and as new data emerges, practices change quickly to build upon whatever new evidence has emerged. The complexity of treatments continue to increase. Overlay the genetic and genomic complexity David described, and you get a sense of the challenges (and opportunities) cancer researchers face in order for science continue to improve outcomes for patients with cancer.
So it’s a bit of a shock when you shift your attention to the alternative medicine “literature”, where simple solutions abound. One that’s popular among patients I speak with, particularly those with European backgrounds, is the use of what are called systemic enzymes – enzymes, consumed orally, with the intent of whole-body effects. These products are not used as part of “conventional” medicine but are popular supplements recommended by alternative practitioners. I was recently asked about a product called Wobenzym N, a product with German roots which is advertised with the following claims [PDF]:
Taking Wobenzym®N as directed will assist several of your body’s key systems. This product supports the musculoskeletal system by promoting health and mobility in joints and muscles, and has been used for many decades. Wobenzym®N supports the circulatory system by promoting vein health. This product also supports the respiratory system and sinus health. Wobenzym®N is used by many people in the support of a balanced immune system and assists in promoting healthy aging. Wobenzym® is safe and effective and has been used by over 100 million people for over 40 years all around the world.
Vague and non-specific claims, and there’s the Quack Miranda warning there, too. But what does Wobenzym N actually do? Other sites promoting its use go much further in their treatment statements, describing use for conditions ranging from Alzheimer’s and angina to multiple sclerosis, prostatitis, respiratory infections and right through the alphabet to uveitis. Some mention utility in treating cancer. What ties all of these disparate conditions together? There is, as is popular in alternative medicine, One True Cause of All Disease. When you’re using systemic enzymes, the OTCOAD is is inflammation.
Rubor, calor, dolor, tumor
Inflammation is our body’s response to infection and injury and is part of the healing process. Diseases with an inflammatory component are common, and have a huge health impact – think of asthma, arthritis, and inflammatory bowel disease, all common, chronic illnesses affecting millions. Low grade inflammation associated with obesity may be the trigger of a number of obesity-related complications. But “inflammation” doesn’t come in one form. There are multiple mediators, such as cytokines and ecosanoids. There’s a wide variety of cellular responses. As Peter Lipson at Science-Based Medicine has observed:
Inflammation is a medical term that refers to a host of complex physiologic processes mediated by the immune system. Inflammation gets its ancient name from the obvious physical signs of inflammation: rubor, calor, dolor, tumor, or redness, heat, pain, and swelling. As the vitalistic ancient medical beliefs bowed to modern science, inflammation was recognized to be far more complex than just these four external characteristics. In addition to being a response to injury and disease, the cellular and chemical responses of inflammation can cause disease. For example, in asthma and food allergies, a type of immune reaction called type I hypersensitivity elicits a harmful type of inflammation. Coronary heart disease, the biggest killer of Americans, is believed to have a significant inflammatory component.
While there can be inflammatory components to many different diseases, it is a gross oversimplification to think that we can treat all forms in the same way, until there’s evidence to show that’s the case. Asthma and arthritis both have inflammatory elements, but they are different diseases with different treatments. But simplify the conditions to just be “inflammation” and you can introduce an equally simple solution. That solution? Systemic enzyme therapy:
Wobenzym®N works by providing “systemic enzyme support,” which describes a process that uses enzymes to assist the body’s various regulatory and communication systems, specifically the immune system.† A balanced immune system is necessary for maintaining overall health. Active enzyme molecules must be readily available in the small intestine to make sure that the systemic effect of the enzymes is achieved.
Enzymes play a critical role in the body and are involved in an astounding number of metabolic processes. Scientists suspect there may be as many as 15,000 enzymes at work in our bodies on a daily basis. Enzymes are involved in a variety of bodily processes including: breathing, growing, digesting, producing energy, conducting nerve impulses, clotting blood, recovering after exercise, or balancing the complex processes of the immune system.
Enzyme supplementation can be science-based. Its use in pancreatic disease is common, as well as diseases like cystic fibrosis. But those are not uses where the enzymes need to be absorbed from the gastrointestinal tract. Systemic enzyme replacement is something different.
I first encountered the idea of massive enzyme superdoses when I learned about the Gonzalez regimen, an alternative cancer treatment regimen discussed at length over at Science-Based Medicine. The treatment includes coffee enemas and hundreds of tablets of pancreatic digestive enzymes daily. The regimen itself was based around the speculation of cancer causes which have now been definitively disproved. A clinical trial of the Gonzalez regimen was funded by the National Center for Complementary and Alternative Medicine (NCCAM), which included a large number of pancreatic enzymes. The results of the trial were remarkable, but not in a positive way for the “alternative” approach: Conventional chemotherapy treatment for pancreatic cancer was three times better than the Gonzalez regimen.
Our pancreas secretes enzymes to help in digesting food. Should we expect that consumed enzymes will be absorbed into the body? Enzymes are large proteins that act as catalysts for biochemical reactions throughout the body – many chemical transformations are catalyzed by an enzyme. Many parameters can affect enzyme activity, including pH and temperature, and the presence of activators and inhibitors. Given the importance of enzymes in the body, genetic disorders that affect enzyme production and function can have catastrophic consequences. We’d also expect that the production and distribution of enzymes in the body would be fairly tightly controlled, given the potential effects, and given the food we eat will have its own share of naturally-occurring enzymes in it, too.
The use of proteins as therapeutic agents to influence disease is one of significant research interest. The challenge in introducing proteins into the body is that most are quickly eliminated from circulation, whether it’s by biotransformation by enzymes or renal filtration. Very large doses may be required, increasing the potential for non-specific toxicity and even allergic reactions. The most common therapeutic uses of proteins is by injection, because large chemical molecules are generally either destroyed by our endogenous digestive enzymes or, if they survive, cannot cross membranes into the bloodstream.
So the concept of giving enzymes orally, and achieve meaningful therapeutic effects in the body, is one with a considerable number of drug design hurdles. Is that occuring? Looking at Wobenzym N, each enteric coated tablet contains:
- Bromelain 45mg
- Chymotrypsin 1 mg
- Pancreatin 100 mg
- Papain 60 mg
- Rutin 50mg
- Trypsin 24mg
The recommended dosage is 3 tablets, twice daily, 45 minutes before meals. Before digging into the clinical data, I wanted to better understand the formulation and the dosing, keeping the design and administration issues in mind.
ADME
Every summary of a drug’s characteristics (the “monograph”) will have the same section. It’s abbreviated ADME which stands for Absorption, Distribution, Metabolism and Elimination. This is the section where behaviour of the the chemical in the body is summarized. This isn’t the clinical section, describing the therapeutic effects. It’s simply characterizing how extensively and how quickly the drug is absorbed from the gastrointestinal tract, where it distributes in the body (the “volume of distribution”) how and if it is broken down or “biotransformed” to make it easier to eliminate, and how quickly it is eliminated from the body. (I described this process in more detail in a previous post on generic drugs.) I want to see this graph, or be presented with enough data to understand what it looks like.
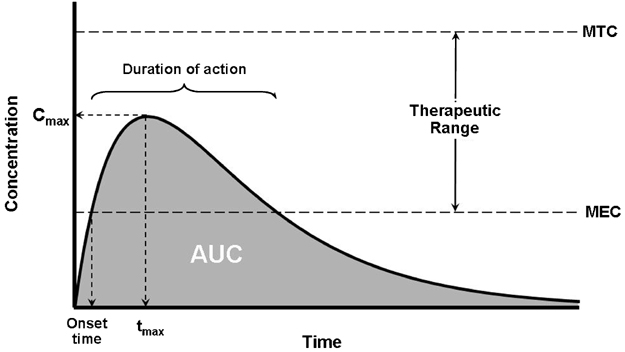
Plasma level curve for a drug
It’s the basic pharmacology work that’s done on a drug that gives us the information to understand its characteristics in the body. There is no point in doing clinical trials of a chemical packaged as a tablet, if we cannot confirm that the active ingredient is actually absorbed when it’s consumed. Clinical trials follow the basic pharmacology work. If the drug is treating different conditions, we may need to study different doses to establish the MEC for each condition. (For example, you need to take a lot more of an anti-inflammatory drug to treat rheumatoid arthritis than you need to treat a headache).
This is the study of pharmacokinetics, and it allows us to determine how the drug should be dosed and delivered in the body. Is it slowly eliminated, so the dosing can be infrequent – daily or even weekly? Is it rapidly eliminated from the body, meaning we need to dose multiple times a day to stay in the sweet spot of the therapeutic range? How is it eliminated from the body? Is it transformed by the liver? What impact does changing the dose have on the elimination of the product? What dose ranging studies have been done on the product that have established the appropriate dose? And how does that dose change, depending on the condition being treated?
My reason for belaboring this points is that understanding the ADME is essential to using drugs, supplements, or chemicals of any kind in a rational way. With herbs, it’s the difference between herbalism and pharmacognosy. Without knowing the ADME, the dosing of any product is empirical – a shot in the dark. Coming back to Wobenzym N, we have a combination product with six different ingredients. The dosing instructions are very specific: 3 enteric coated tablets, twice daily, 45 minutes before meals. It’s the same for all of the different reasons for use described. But why this dose? Why 3 tablets? Why twice daily? What happens if you take more, or less? Different ingredients typically have their own physicochemical characteristics. What effects does each have? I looked at each ingredient first in the Natural Medicines Comprehensive Database (NMCD), and then in the primary literature itself. Here’s what I could find:
- Bromelain is a term used for a collection of enzymes isolated from pineapple. While it’s rated by NMCD as “possibly effective” for osteoarthritis, the data are contradictory with some studies suggesting it has no effect on osteoarthritis. It has not been well demonstrated that bromelain reaches any clincially meaningful concentration in the blood. These are large protein molecules and it’s not clear how effectively they are absorbed – doses of 3000mg/day seem to result in tiny, albeit measurable, blood levels. Blood plasma components may inactivate any bromelain that is absorbed, though a half-life has been described [PDF]. On balance, the data are not impressive.
- Chymotrypsin is a protein-digesting enzyme that is synthesized and secreted by the pancreas. I could locate no published efficacy of supplemental single ingredient chymotrypsin for any condition. It’s not clear what a supplemental dose of a few milligrams would have. I couldn’t locate any information that characterizes its ADME.
Pancreatin is a mix of digestive enzymes including lipase, protease, and amylase, is used as prescription drug to treat pancreatic insufficiency, in conditions like cystic fibrosis. High doses have been linked to increases in blood/urine uric acid levels. There is no well-established use of oral pancreatin for anything other than pancreatic inefficiency. Again, little information exists to describe the ADME.
Papain is a papaya-derived combination of enzymes. I could find a single study (in German) which compared oral supplements favourably to acyclovir for herpes zoster pain. Given the limited info in the abstract, it’s not possible to evaluate the data more fully. Little data exists to characterize the ADME.
Rutin is a flavenoid rated as “possibly effective” for osteoarthritis on the basis of a single double-blind trial of an enzyme product (bromelain, trypsin, and rutin) versus diclofenac. Rutin does not seem to be absorbed intact, through it appears to elevate plasma levels of quercetin, and seems to have an effect on the absorption of other drugs. Again, little information exists to understand the pharmacokinetics. - Trypsin is another enzyme produced in the pancrease for digestion of proteins. Beyond the trial with rutin, I could locate no published trials evaluating efficacy for any other condition. Limited information exists to describe the ADME.
As I noted, getting large proteins like enzymes to be absorbed is a drug design challenge. Even if absorbed, how large molecules would escape rapid metabolism and elimination isn’t clear, either. With the ingredients in Wobenzym N, there appears to be some data to suggest that some components do reach the bloodstream. And there are some studies with the individual ingredients – but nothing that unequivocally establishes a meaningful effect. With that in mind, I looked for studies using the Wobenzym combination of ingredients.
The studies
I stared a review with the Natural Medicines Comprehensive Database (NMCD). Regarding Wobenzym N, it says, in part:
Wobenzym N is promoted for reducing inflammation and edema, and speeding recovery from certain injuries. Often it is used by individuals with arthritis and by athletes, including some professional and Olympic athletes. Enzymes in this product are thought to activate macrophages that attack inflammation-causing circulating immune complexes. Rutoside, an additional ingredient, acts as an antioxidant. To date there is no convincing clinical evidence that Wobenzym is effective for these uses. Because these enzymes do not affect prostaglandin synthesis, Wobenzym N is also promoted to be free of many of the side effects associated with non-steroidal anti-inflammatory drugs (NSAIDS). Adverse reactions reported after oral administration include loose stools, increased gas, and skin reactions.
NMCD cautions that there is also potential for the product to affect blood coagulation.
Are there clinical trials with Wobenzym? Yes, but few are in English, which complicates the review. I could locate no evaluable trials in PubMed, but other websites list trials in conditions such as pelvic inflammatory disease, cancer, and multiple sclerosis. Some therapeutic improvements have been attributed to the consumption of Wobenzym (e.g., diabetes, post-heart attack) but the studies are preliminary, sometimes unblinded, and don’t appear to be duplicated. One of the few English papers appeared in Medical Hypotheses, not a good sign for someone seeking science-based medicine. There’s an uncontrolled trial in bronchitis in children, in a study published in Russian. Other studies are published in Czech, Ukranian, Latvian, and Russian. One German systematic review declared “oral proteolytic enzyme treatment does not offer a justified alternative in comparison with NSAID in the anti-inflammatory treatment of rheumatic disease.” Overall, no large clinical trials with relevant clinical outcomes, and no persuasive evidence to demonstrate clinically meaningful effects for any single condition it is used to treat. On balance, the safety profile of the product seems acceptable, but it’s not clear how extensively safety data was captured in these small trials.
There are several trials with a similar product, Phlogenzym (rutoside, bromelain and trypsin). One didn’t suggest impressive results for ankle strains. A trial studying the same combination for hip osteoarthritis suggests non-inferiority with diclofenac, and an open-label trial for osteoarthritis of the knee found non-inferiority as well. I even found a small trial declaring it effective for treating pediatric sepsis, which left me curious if there are research ethics boards in India.
There is also the interesting case of the enzyme serrapeptase, also sold as an anti-inflammatory. Sold by the pharmaceutical company Takeda since 1968 for asthma, bronchitis, and touted as an enzyme anti-inflammatory for a large number of other uses, it was withdrawn from the Japanese market in 2011, after double-blind trials concluded that it had no therapeutic effects.
On balance, looking at the data for systematic enzymes, I wasn’t impressed. Despite the generalized claims of effectiveness, there are so many limitations in the data itself it’s not clear we can infer that the treatment effects are real. And given the lack of data on the absorption, distribution, metabolism and elimination of Wobenzym, it’s not clear that this product is even absorbed to a meaningful extent and available in the body to have systemic effects. Without any objective measure to evaluate efficacy, it’s not clear that supplementation will have any meaningful therapeutic effects for any condition, chronic or otherwise. You may feel better when you take it, but there’s no persuasive evidence yet that it’s having a meaningful effect.
This rock keeps tigers away
It would be an amazing discovery – Nobel worthy – if there were an oral therapy with demonstrably beneficial effects on a variety of chronic diseases without evidence of toxicity. Even demonstrating that large protein molecules can be consumed orally and be delivered in significant amounts to the bloodstream would be notable. Unfortunately, neither have been convincingly demonstrated with Wobenzym or other “systemic” enzyme treatments. Science is complicated, and simple solutions may be attractive, but they’re also quite possibly wrong. Given the weak clinical and pharmacokinetic data for this product, I expect that, should more research be done, it will follow the same evidence trajectory of many other supplements with an implausible premise: As the research studies improve in size and methodologic rigor, the treatment effects will disappear. Until better evidence appears to demonstrate the efficacy and safety of systemic enzyme therapy, their use can’t be considered science-based.

Nice post. One important consideration is that the consumption if proteolytic enzymes, as well as lipases and amylases, may lead to pancreatic atrophy in the long term. This concern, along with a complete lack of evidence for any therapeutic effect, has lead Health Canada to recommend that all enzyme products carry a label saying that their uses should be restricted to periods no longer than 3 days. http://www.drterrywillard.com/wp-content/uploads/2011/09/Consultants-Final-Report_Enzymes.pdf is the NHPD’s consultant report on such products. This is is still in the comment period as far as I know – for another couple of weeks at least.
” it was withdrawn from the Japanese market in 2011, after double-blind trials concluded that it had no therapeutic effects.”
How nice that the Japanese can take action when evidence warrants. No matter how many trials show CAM to be useless, we can’t get anything done here that is based on science–instead we fund the continued testing of products and treatments, and then require the NIH to post these “results” couched in language that allows just enough leeway for the believers to pretend that it is legitimate.
Thanks for taking this product apart so thoroughly.
so if enzyme therapy is useless? how does the product ‘Bean-o’ work?
Beano contains alpha galactosidase which works entirely in the intestine, and is claimed to support the breakdown of complex carbohydrates. It is not absorbed, and is therefore not a “systemic” enzyme replacement.
Bromelain treatment decreases secretion of pro-inflammatory cytokines and chemokines by colon biopsies in vitro.
Doesn’t this study from Duke University suggest positive benefits of bromelain?
I would suggest the author is guilty of what he or she accuses alternative medicine of. That is offering up equally simple solutions which are positioned as still being within the realm of science. This approach allows the practitioner to ignore all of the complexity and difficulty of practicing real medicine, yet offer nostrums that, on first glance, can sound legitimate. Science-y, even.
I find the tone of the author to be of someone with limited intelligence who likes to sound impressive but really is just a voice among millions. The vast complexity of human experience as it relates to health will not be conquered by me or the author.
Electronic health records and human genomic patient information will ultimately solve many of these questions from a statistical standpoint. This should lead to individualized medicine at an unprecedented level (for those who can afford it). How is that for alternative medicine? Understand doctors are not the ones that have perspective, they are merely implementators of a particular brand of science who can also develop their own experience which can affect outcomes. Its similar to my profession, civil engineering. I’ve dated a cancer researcher from UCSF, chief medical officer/surgeon for John Hopkins, biochemistry university professor at Cal Poly San Luis Obispo, and now a pediatrician as well as suffered from several conditions doctors were unable to help with. I am a genius, but have less intelligence than millions. The truth of the matter is, there is much doctors don’t know, yet most are unwilling to accept this as a position, its too unsettling for them.
Well said. Author says that there are studies done in other languages, but since he’s too lazy to get the interpretation, he’s going to ignore that data and find and mention all the quick faulty data. So far it works for me and chronic back pain. Use that data!
That’s not data, it’s anecdote and there are several possibilities for your “results”; placebo effect, benefit from something else you did at the same time, spontaneous healing–things getting better on their own regardless of “treatment”.
I have endometriosis and ever since I’ve been taking Wobenzym, I’ve been pain free, which is huge. I can’t tell you how it works, but it does.
You missed this study on Pubmed: http://www.ncbi.nlm.nih.gov/pubmed/7663574
Thanks for posting this Wonemzym study.
When I first visited my Urologist, he absolutely assured me that sawtooth palmetto, etc. did not work, that there was no scientific evidence that it worked. Two years later, having heard an overwhelming amount of anecdotal evidence from his prostatitis patients, he told me that I should DEFINITELY be taking palmetto and pygeum.
Kevin Smith
Get a new (science-based) doctor.
Have you considered the side effects of immunosuppressants for rheumatoid arthritis, or the side effects long term use of NSAIDS? They are pretty severe, yet doctors glibly prescribe them!
@Jillian
I have a child and a grandchild with RA. Both are receiving standard treatment. Both are doing well. We fully realize that these are serious medications, but that’s why we have good doctors to monitor the patients and make sure they are doing well. There were long discussions in both cases, and nothing “glib” about it at all.
In both cases, the medications have enabled them to get on with their lives and livelihoods, nearly pain free. Given that neither could hardly walk or get out of bed, they are grateful for these advances in pharmacology.
My job, as head of this family, is to follow smart and educated people such as Scott G. to make sure people I love are not parted with their hard-earned money by quacks and quackademic “medicine”.
Eastern medicine was around long before western medicine. Many of these supplements come from eastern medicine ideas. I too have rheumatoid arthritis. I take Remicade for it but still have many more pains. Right now, I prefer Wobenzym N over 12-16 advil a day. Advil can cause stomach ulsers and phantom pain. Go with what you feel is best for you and your family. You dont need to hate and calk names to what you don’t understand. I will look for what I feel is best for me. Sending prayers for your family’s health.
Curious about your categorization of Wobenzym, which is German-invented and first produced in the 1960s. You don’t get more “western” than Germany.
@Michelle
There is really no such thing as Eastern “Medicine”, only Eastern superstition and faith-healing. Modern people, in the east, when faced with any real illness, flock to real doctors–even if they also persist in their use of culturally-ingrained belief-based healing traditions.
Call it any rude word your mind can come up with. Give it any excuse for working that you want. Every “science based” medicine does not work for everybody. Remicade works for me, but not for others. Sometimes Remicade works for years and then stops. I’ve had Rheumatoid Arthritis for 13 years now. I know all about the waves of feeling good and feeling bad, so I confidently say that Wobenzym works for me as good as Advil, Aleve, etc. If I say something (Wobenzym) works for me to some extent, who are you to determine that it’s not true? I’m not claiming that it takes the place of Remicade, not that it should concern you. Nobody is making you use it on yourself or your family, so I don’t really understand your strong objections to what others say work for them.
Really, no matter how you put it, every medicine we put into our body is some chemical that has some side-effect. Just because Remicade or Advil is proven scientifically to work in x% of the cases when tested by the company that creates it, does not negate the fact that these medications still can and do have adverse side effects. Trying to find ways so you don’t have to constantly put the same thing into your body is something I view as a good alternative.
@Parent:
“If I say something (Wobenzym) works for me to some extent, who are you to determine that it’s not true?”
We are asking that all health treatments be subjected to the best method we have for determining the truth of their efficacy: science-based medicine. It does not seem to measure up at the moment, and thus shold not be available for sale. You of all people, knowing the variability of arthritis, should understand how unreliable personal anecdotes are, and thus why the more rigorous approach of science is needed.
Further, we have legislated standards based on best science for all kinds of products, from soup to cars. We don’t let people try out soup or cars that have not been subjected to these standards on the basis that they think it could or did work for them. Surely, that should apply even more stringently to health treatments.
“Science” based medicine does not know everything, and what it does it purveys with outdated theories. All major theories in medical science are wrong ( in all of science indeed). How do you explain the lack of clinically significant trials on natural products ( non patentable) ? I think big pharmaceutical companies own you and your science. When you get really sick, and I’m sure you will, purely out of drug side effects, I’m sure you will look at the real science that is without big pharma interest. There are hundreds of s ridiculous claims in the literature which amount to scientific fraud. Look at the statin combo drug vytorin by Merck 🙂 . You need to wake up my boy. But why admit it when your paid n owned . All in all I would grade this attempt of truth disfigurement as a 6 out of 10.
Thanks Aman. From my perspective (caregiver to someone diagnosed with liver cancer 7 years ago) all I can do is suggest products and protocols. Some have a positive impact. some make symptoms worse. Reading studies and literature may have its place but ultimately we need to ask the patient “do you want to try this?”
Hopefully the patient will still have the capacity to respond.
Overall, we are choosing processes, protocols that are non-toxic because we are dealing with the liver. Even herbs can cause an adverse reaction. But prescription drugs do not work. They are toxic to this patient and it doesn’t matter what the literature or sales rep says.
“Reading studies and literature may have its place but ultimately we need to ask the patient ‘do you want to try this?’ ”
I think the ethical approach as a caregiver has to be to review the literature as well as the recommendations of competent health authorities on treatments and to recommend only those that meet the highest standards of science.
“But prescription drugs do not work. They are toxic to this patient and it doesn’t matter what the literature or sales rep says”
I am rendered almost speechless. I guess all those people taking antibiotics have been deluding themselves all these years…
“I think big pharmaceutical companies own you and your science”
“But why admit it when your paid n owned”
Nothing like the faulty logic of the pharma shill gambit.
“Look at the statin combo drug vytorin by Merck”
Because other pharmaceuticals do not work, “natural” products do or some other product does work? More faulty logic.
“How do you explain the lack of clinically significant trials on natural products?” How do you explain the lack of the lack of trials by companies making money off of “natural” products? One would think that companies making a profit off of a health product would have solid, scientific evidence to back up their sales. To do otherwise would be ethically fraught.
Much “science based” medicine these days produced by big pharma is researched by big pharma, and then approved by FDA officials who were once part of big pharma or receiving $$$ from big pharma.
That’s $$$ based, not science based.
There is a lot of junk in the pharmacy that should be illegal.
Every natural product has some kind of organic compound that affects us, and they may or may not work, but should not be automatically debased by people who have a grudge against “homeopathy”, as some commenters above seem to have.
The study that was cited about the enzymatic therapy cancer treatment was true. The natural protocol did not fare as well. The problems with that study are reflective of my concerns about other attempts at unbiased studies of possible alternative therapies. In that study everything possible was done to tilt the table so that the accepted medical protocol would be favored, including a rush to publication under protest so I guess it could be more available to detractors. Even the patient selection process was controlled by the accepted protocols developers who should have never been involved if the trial was to be random. The patients selected for the alternative therapy were decidedly more advanced. Patients who were to recieve the alternative therapy had their treatment delayed by as much as 6 weeks while the accepted therapy was begun at times within hours. Yet this study is quoted as good science and peer reviewed. You speak as though these studies have messeanic quailities. They do not. Having been involved in healthcare for sometime and watching the political abilities of the drug industry over 40 years, there is little hope that an alternative to drugs will ever see the light of day while medications that perform slightly better than placebos will be hailed with great acclaim as miraculous. $$$$$$$$$$ To say that all drugs are simply poison in inaccurate. To dismiss all alternative therapy as placebo and superstition is equally lame.
Well, I don’t know why products like serrapeptase & wobenzym work form some people and not others but I have had chronic sinusitis for over 10 years and I took serra-plex for 3 weeks and it cleared it right up. I also had a very painful ovarian cyst which was resolved during the same period I was so happy with the results I started combining wobenzym and serrapeptase to see if it would get rid of a polyp and fibroids. I won’t know for two weeks if it was successful on the polyp but if its not I will be sure to report back here